Intra bony defect
What would you do ?
- Intro
- Key scientific data
- Clinical tips
Intro

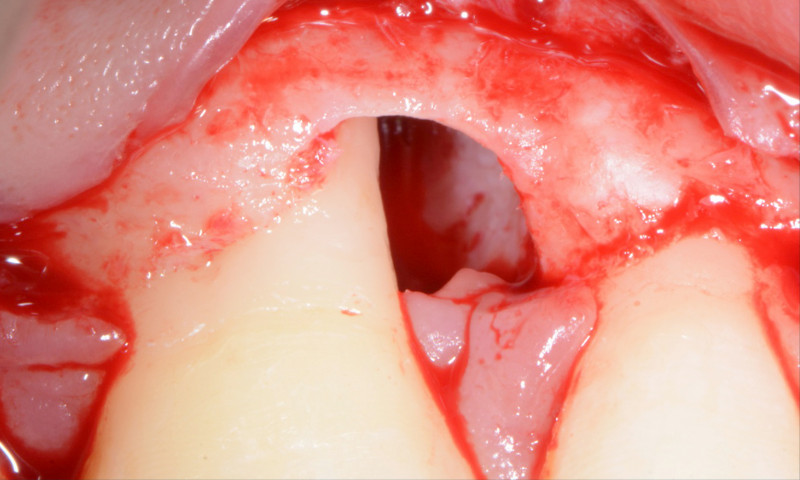
Periodontal defect with an intrabony component is a common finding in patient affected by severe periodontitis (stage 3 and 4).
After a cause related therapy, a surgical approach is often required to reduce the pocket depth and the intrabony component.
Regeneration is commonly recommended for intrabony defect of 3mm or more, using either biologic products or barrier membrane alone or associated with bone substitute.
Key scientific data
→ Evidence indicates that periodontal regeneration is a predictable procedure for the treatment of isolated and multiple intrabony defects.
→ Periodontal regenerative therapy in intrabony defects results, in general, in shallower residual pocket depth and larger clinical attachment level gain compared with flap, translating in high rates of tooth survival, on a medium (3-5 years) to long-term basis (5-20 years).
Regeneration is commonly recommended for intrabony defect of 3mm or more, using either biologic products or barrier membrane alone or associated with bone substitute.

Variability of the outcomes in different studies may be explained by :
- Patient-related factors : smoking habit, compliance with home oral hygiene and residual inflammation after cause-related therapy.
- Defect-associated factors : defect depth and radiographic angle, number of residual bony walls, pocket depth and the degree of hypermobility
- Surgical-related variables : surgical skill, clinical experience and knowledge
→ Periodontal regeneration can change the prognosis of hopeless teeth and is a less costly alternative to tooth extraction and replacement
Clinical tips
→ Efficient cause related therapy : plaque and bleeding index below 20% and adequate soft tissue consistency in the area of the scheduled surgery

→ Minimally invasive surgical approach (MIST or M-MIST) based on the intrabony component location and anatomy
→ Enamel matrix derivative alone in narrow intrabony defect
→ Enamel matrix derivative in combination with xenograft (porcine or bovine origin) or autogenous bone graft in wide intrabony defect (wide radiographic angle) with no soft tissue support but sufficient bony wall. Despite promising outcome, further studies are required to support the combination of enamel matrix derivative with cross-linked collagen sponge in wide intrabony defect.
→ In the esthetic zone, a connective tissue graft is strongly recommended (either suture to the periosteum or to the inner part of the buccal flap) to improve the soft tissue volume and reduce the post operative recession
→ Regular supportive periodontal therapy tailored to each patients risk factors is mandatory after regenerative surgery